| Cloud-Native & Serverless | ✅ Fully serverless, stateless, auto-scalling | ❌ Stateful, always-on | ❌ Stateful, always-on |
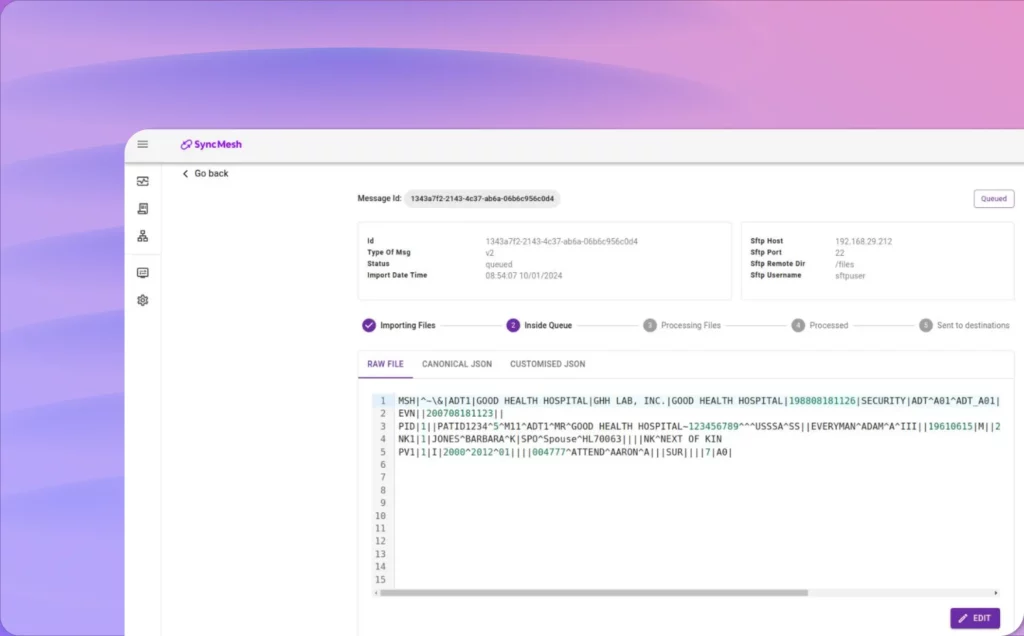
| Incremental Message Processing | ✅ Native support for message-by-message processing | ⚠️ Channel-based (indirect support) | ⚠️ Limited Support |
| Schema Validation & Type Safety | ✅ Strongly enforced schema and static typing | ⚠️ Limited; custom scriptiing | ❌ Minimal |
| Transformation Model | ✅ Schema-driven, declarative mappings | ⚠️ Script-based or GUI-driven | ⚠️ Script-based (JavaScript) |
| Developer Workflow | ✅ Fast, self-service, low vendor dependence | ⚠️ Medium-DUI-driven | ❌ Slow, vendor-led |
| Cost Model | ✅ Pay-per-utilization; no idle infra | ❌ Requires provisioning; always-on | ❌ Requires provisioning; always-on |
| Architecture | ✅ Microservices; composable & modular | ❌ Monolithic | ❌ Monolithic |
| UI & Observability | ✅ Optional UI; deployable without it | ❌ Required | ❌ Required |